
Serratia spp.
Pathogen Safety Data Sheets: Infectious Substances – Serratia spp

NAME: Serratia spp.
SYNONYM OR CROSS REFERENCE: Serratia, S. marcescens (Serratia pattern 1, Serratia biotype 1, phenon A), S. liquefaciens, S. entomophila, S. ficaria, S. fonticola, S. glossinae, S. grimesii ,S. marcescens (S.
marcescens ss marcescens and S. marcescens ss sakuensis) S. nematodiphila , S. odorifera, S. plymuthica, S. proteamaculans (S. proteamaculans ss proteamaculans, S. proteamaculans ss quinovora), S. rubidaea, S.
ureilytica Footnote 1, Footnote 2.
CHARACTERISTICS: Serratia spp. are chemoorganotrophic, facultative anaerobic bacteria with low nutritional requirements, and belong to the Enterobacteriaceae family Footnote 3.
They are gram negative rods, 0.9-2 µm long and 0.5-0.8 μm in diameter Footnote 2.
They possess peritrichous flagella that allow them to swim and swarm (with differentiation), and are ubiquitous in soil, water, and plant surfaces.
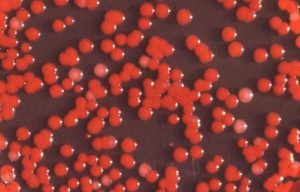
Many species produce a red to pink pigment, named prodigiosin, which is easier to observe in phosphate-free medium incubated at 30°C rather than 37°C Footnote 3.
This pigment is suspected to have antibiotic, potent immunosuppressive, proapoptotic, and anticancer properties, while its role for Serratia spp. is still unknown Footnote 2. S.
marcescens produces a biofilm, with unique cellular and structural differentiation characteristics to those of the standard biofilms produced by Pseudomonas aeruginosa and Escherichia coli.
The latter bacteria produce biofilms, which only consist of microcolonies of undifferentiated cells. Serratia spp. also produces β-lactamases. All of the former metabolic processes are controlled by quorum sensing. S. marcescens ssp. sakuensis is able to produce endospores, but other members of the genus are not Footnote 4.
SECTION II — HAZARD IDENTIFICATION
PATHOGENICITY/TOXICITY: Serratia spp. are opportunistic pathogens and are one of the ten most common causes of bacteremia in North America Footnote 5.
They are responsible for a variety of infections, including bacteremia, pneumonia, intravenous catheter-associated infections, osteomyelitis, endocarditis, and, rarely, endogenous and exogenous endophthalmitis Footnote 2, Footnote 6.
Symptom of endophthalmitis appears rapidly after infection, and may include fever, erythema, ocular pain, periorbital swelling, and hypopyon (pus in the eyes). The mortality rate from bacteremia due to Serratia spp. 6 months after infection is 37% Footnote 7.
Serratia infections in neonates are frequent (11-15% in neonatal intensive care unit) and may include bloodstream infection (42%), conjunctivitis (26%), pneumonia (13%), urinary tract infection (8%), meningitis (7%), and surgical site infections Footnote 8.
Other infections in infants are documented (otitis externa, enterocolitis and omphalitis, gastroenteritis, septic arthritis, and intraperitoneal infection/abcess), but are rare. Risk factors include birth weight, use of mechanical ventilation, and gestational age (under 37 weeks are at greater risk).The mortality rate in neonates is 44%.
EPIDEMIOLOGY: Worldwide distribution Footnote 3. Biotypes, serotypes and biogroups may be region-specific. Sporadic infections are considered endemic.
Epidemics may be caused by contact with a common source by multiple patients, or by patient-to-patient contact. The intestinal tract of newborns may also be infected. S.
marcescens non-pigmented strains are more ly to cause an infection than pigmented strains Footnote 9.
Until recently, Serratia was considered to be a mostly nosocomial pathogen Footnote 7, Footnote 10. In 2007, a study in the Calgary health care region (Canada) demonstrated that 65% of infections with Serratia species were actually of community origin. According to the same study, 10.8 per 100,000 inhabitants are carrying the pathogen and 0.9 per 100,000/year develop bacteremia.
The rate of Serratia isolation is higher in those over 60 years of age. In the under 60 population, the rate of isolation in men and woman are slightly different (65.9 per 100,000 in men and 36.5 per 100,000 in women). The difference in isolation is mostly observed for hospital-acquired infection. There is no seasonal or yearly variation in incidence.
92% of isolates were Serratia marcescens, 4% S. liquefaciens, 1% S. odorifera and 1% S. rubidaea. Other isolates included S. fonticola, S. plymuthica, and nonspeciated Serratia (2%). Bacteremia was usually caused by S. marcescens (88%) and S. liquefaciens (7%). S. odorifera (2%) and nonspeciated Serratia also have caused bacteremias.
Men over 60 years of ages were most susceptible to developing bacteremia.
HOST RANGE: Plants and animals (including human) have been found to be hosts to the different Serratia spp. Footnote 3.
INFECTIOUS DOSE: Unknown.
MODE OF TRANSMISSION: Ingestion of contaminated foods and direct contact Footnote 3. Nosocomial transmission may occur by hand contact from hospital personnel and other patients. Fomites may also spread Serratia.
INCUBATION PERIOD: Unknown.
COMMUNICABILITY: Serratia may be directly transmitted from person-to-person, but rates are unknown Footnote 3.
SECTION III — DISSEMINATION
RESERVOIR: Soil and animal (including human) are considered reservoirs Footnote 3.
ZOONOSIS: None Footnote 3.
VECTORS: None Footnote 3.
SECTION IV — STABILITY AND VIABILITY
DRUG SUSCEPTIBILITY: Serratia spp. are usually susceptible to aminoglycosides, fluoroquinolones, and co-trimazole Footnote 7.
DRUG RESISTANCE: Many Serratia spp. isolates (39-73%) are resistant to gentamicin Footnote 7. They are all resistant to penicillins and cephalosporin.
SUSCEPTIBILITY TO DISINFECTANTS: Phenolic disinfectants, 1% sodium hypochlorite, 70% ethanol, formaldehyde, glutaraldehyde, iodophore, and peracetic acid are effective against Serratia spp. Footnote 11.
PHYSICAL INACTIVATION: Serratia spp. are inactivated by UV, microwave, gamma radiation, moist heat (121°C for at least 20 min), and dry heat (165-170°C for 2 h) Footnote 12-Footnote 15.
SURVIVAL OUTSIDE HOST: S. marcescens may survive from 3 days to 2 month on dry, inanimate surfaces, and 5 weeks on dry floor Footnote 16.
The organism may survive less than 4 days in a blood bag under aerobic conditions and 20 days in semi-anaerobic/anaerobic conditions Footnote 17.
It has been also reported to survive in contact lens disinfectant (with chlorheximide), double-distilled water, non-medicated hand soap, but no duration has been reported for those cases Footnote 18-Footnote 20.
SECTION V – FIRST AID / MEDICAL
SURVEILLANCE: Monitor for symptoms and perform bacteriological isolation and serotyping/biotyping Footnote 3.
FIRST AID/TREATMENT: Give appropriate antibiotherapy Footnote 3.
IMMUNIZATION: None currently available.
PROPHYLAXIS: None currently available.
SECTION VI — LABORATORY HAZARDS
LABORATORY-ACQUIRED INFECTIONS: 5 laboratory acquired infection with S. marcescens have been reported as of 1999 Footnote 11.
SOURCES/SPECIMENS: Serratia spp. are found in feces, wound exudates, respiratory specimen, blood, eye culture, and urine Footnote 10.
PRIMARY HAZARDS: Accidental parenteral inoculation, droplets exposure of mucous membrane, infectious aerosols, and ingestion Footnote 11.
SPECIAL HAZARDS: None.
SECTION VII – EXPOSURE CONTROLS / PERSONAL PROTECTION
RISK GROUP CLASSIFICATION: Risk Group 2. This risk group applies to the genus as a whole, and may not apply to every species within the genus.
CONTAINMENT REQUIREMENTS: Containment Level 2 facilities, equipment, and operational practices for work involving infectious or potentially infectious materials, animals, or cultures.
PROTECTIVE CLOTHING: Lab coat. Gloves when direct skin contact with infected materials or animals is unavoidable. Eye protection must be used where there is a known or potential risk of exposure to splashes Footnote 21.
OTHER PRECAUTIONS: All procedures that may produce aerosols, or involve high concentrations or large volumes should be conducted in a biological safety cabinet (BSC). The use of needles, syringes, and other sharp objects should be strictly limited. Additional precautions should be considered with work involving animals or large scale activities Footnote 21.
SECTION VIII – HANDLING AND STORAGE
SPILLS: Allow aerosols to settle and, wearing protective clothing, gently cover spill with paper towels and apply an appropriate disinfectant, starting at the perimeter and working towards the centre. Allow sufficient contact time before clean up.
DISPOSAL: All material should be decontaminated before disposal with steam sterilization, incineration or chemical disinfection.
STORAGE: Samples and biological material should be store in appropriately labelled sealed containers.
SECTION IX — REGULATORY AND OTHER INFORMATION
REGULATORY INFORMATION: The import, transport, and use of pathogens in Canada is regulated under many regulatory bodies, including the Public Health Agency of Canada, Health Canada, Canadian Food Inspection Agency, Environment Canada, and Transport Canada. Users are responsible for ensuring they are compliant with all relevant acts, regulations, guidelines, and standards.
UPDATED: December 2011
PREPARED BY: Pathogen Regulation Directorate, Public Health Agency of Canada.
Although the information, opinions and recommendations contained in this Pathogen Safety Data Sheet are compiled from sources believed to be reliable, we accept no responsibility for the accuracy, sufficiency, or reliability or for any loss or injury resulting from the use of the information. Newly discovered hazards are frequent and this information may not be completely up to date.
Copyright ©Public Health Agency of Canada, 2011
Canada
Источник: https://www.canada.ca/en/public-health/services/laboratory-biosafety-biosecurity/pathogen-safety-data-sheets-risk-assessment/serratia.html
Serratia marcescens — Infectious Disease and Antimicrobial Agents

Once considered a harmless saprophyte, Serratia marcescens is now recognized as an important opportunistic pathogen combining a propensity for healthcare-associated infection and antimicrobial resistance.
Serratia marcescens is a member of the genus Serratia, which is a part of the family Enterobacteriaceae. Currently 14 species ofSerratia are recognized within the genus, eight of which are associated with human infection (67).
Of the eight species implicated in clinical infection S. marcescens, S. liquefaciens and S. odorifera are best known (31, 67). Of all Serratia species, S.
marcescens is the most common clinical isolate and the most important human pathogen.
S. marcescens is credited with a long fanatical history dating back to antiquity, when, because of its ability to produce a red pigment it was described as having ‘masqueraded’ as blood (36). Early in this century, this distinctive red pigmentation of S.
marcescens, combined with an apparent low level of virulence, led to its use as a biological marker of infection. Consequently, S. marcescens was used in a number of classic bacterial transmission experiments, which led to improved understanding of the epidemiology of infection (124).
Under more controversial settings, S. marcescens was also used by the US military in a series of biological warfare test experiments conducted on the general population (124). From 1960 onwards, however, non-pigmented isolates of S.marcescenspredominated over pigmented strains in the clinical setting and were increasingly implicated in healthcare-associated infection (24,30) particularly among compromised patients.
As members of the Enterobacteriaceae family, Serratia spp are motile, non-endospore forming Gram-negative rods.
In the laboratorySerratia are routinely isolated from bloodstream and wound sites using blood agar culture or from respiratory and urinary sites using selective culture methods.
Common selective agar cultures include MacConkey agar which categorizes Serratia isolates with the other non-lactose fermenting Enterobacteriaceae or chromogenic agars, which classifies them into a broad Klebsiella, Enterobacter,Serratia and Citrobacter (KESC) grouping (13, 17).
Phenotypically Serratia is one of the easiest genera to differentiate within the Enterobacteriaceae family. Un other enterobacteria, strains of Serratia usually produce extracellular deoxyribonuclease (DNase), gelatinase and lipase and are resistant to the antibiotics colistin and cephalothin.
Traditionally, Serratia spp were identified using the Analytical Profile Index (API) 20E (bio-Merieux) phenotypic microbial identification system (40). With the widespread introduction of automated identification systems, laboratory identification of Serratia spp.
is now routinely performed using systems including Vitek 2 (bio-Merieux), Microscan Walk-Away (Dade-Behring, Siemens), or BD Phoenix (BD Diagnostics, Sparks) (71).More recently, species level identification of Serratia isolates has been successfully achieved using rapid, automated MALDI-TOF MS (matrix-assisted laser desorbtion/ionization time-of-flight mass spectrometry) identification systems (86, 95).
EPIDEMIOLOGY
Serratia marcescens is an opportunistic pathogen whose clinical significance has been appreciated only in the last four decades. While S.
marcescens is a rare cause of community-acquired infections, it has emerged as an important nosocomial healthcare-associated pathogen and a frequent source of outbreaks of hospital infection (72), in both adult (122) and paediatric patients (115).
Results from a recent surveillance programme in the US and Europe, indicate that Serratia spp., accounts for an average of 6.5% of all Gram negative infection in Intensive Care Units (ranked 5th amongst Gram negative organisms in ICU) and an average of 3.5% in non-ICU patients (91).
Currently Serratia is the seventh most common cause of pneumonia with an incidence of 4.1% in the US, 3.2% in Europe and 2.4% in Latin America (51), and the tenth most common cause of bloodstream infection with an incidence of 2.0% amongst hospitalized patients (2).
S. marcescens is rarely associated with primary invasive infection. It operates as a true opportunist producing infection whenever it gains access to a suitably compromised host.
Patients most at risk include those with debilitating or immunocompromising disorders, those treated with broad-spectrum antibiotics and patients in ICU who are subjected to invasive instrumentation. The indwelling urinary catheter is a major risk factor for infection. The risk of a catheterized patient becoming infected with S.
marcescens has been directly related to the proximity of other catheterized patients colonized or infected with the organism (68). The respiratory tract is also recognized as a major portal of entry with S. marcescens being isolated from the respiratory tract of up to 80% of post-operative patients developing S. marcescens bacteremia (125).Not surprisingly, common infections include urinary tract infection in patients with indwelling catheters, respiratory tract infection in intubated patients and bloodstream infection in post-surgical patients, especially in those with intravenous catheters.
CLINICAL MANIFESTATIONS
S. marcescens is implicated in a wide range of serious infections including pneumonia (51), lower respiratory tract infection (112), urinary tract infection (53), bloodstream infection, wound infection and meningitis (72, 74). The organism has also been described as an important cause of ocular infection with high incidence in contact lens-related keratitis (4, 21, 92).
S. marcescens is also a rare cause of endocarditis. In the 1970s, S. marcescens was the most frequent cause of Gram-negative endocarditis among intravenous drug addicts in San Francisco (73).
The frequency has since subsided, although sporadic cases ofSerratia endocarditis still occasionally occur with two of the highest risk groups including intravenous drug users and patients undergoing prosthetic valve surgery.
Skin and soft tissue infections are also unusual although rare cases of invasive cellulitis and necrotizing fasciitis have been reported (60). Septic arthritis has also been reported following diagnostic and therapeutic intra-articular injections (76).
Over the years, S. marcescens infection has been attributed to many different sources.
Outbreaks of infection have been traced to medical equipment including nebulisers (87), bronchoscopes (82), electrocardiogram leads (100), laryngoscopes (20) and contaminated solutions such as inhalation medications (112), prefilled heparin syringes (8, 103), saline solutions (105), parenteral nutrition (3) and antiseptics (76). Many diverse environmental sources such as air conditioning units (82), urine-collecting basins (122), bed-pan macerators (42), liquid soap dispensers (104) and even tap water (46) have also been implicated.
Outside of environmental sources, hospital patients have also been recognized as a reservoir for infection. The gastrointestinal tract is recognized as the predominant site of colonization for S.
marcescens, as is the case for most members of the Enterobacteriaceaefamily. Studies have shown, however, that rates of S. marcescens gastrointestinal carriage are largely dependent on the population screened (11).In the healthy host and non-infected immunocompetent patient, carriage rates remain low (
Источник: http://www.kaupa-tool.com/b26.asp
Serratia spp.—A Practical Summary for Controlling Mastitis

The implementation of control measures for contagious mastitis pathogens has successfully reduced the prevalence of these organisms in U.S. dairy herds. However, dairy producers continue to struggle with the control of environmental pathogens.
Serratia spp. are Gram-negative bacteria, similar in structure to Escherichia coli and Klebsiella spp. The most common mastitis-causing species is Serratia marcescens.
However, the treatment and control of these organisms is similar across all species of Serratia.
Please check this page first if you are interested in organic or specialty dairy production.
Where are these organisms found?
Commonly, these organisms are found in soil and plant matter (including feed).
Therefore, cows on pasture or cows housed on organic bedding material may be at an increased risk for mastitis caused by Serratia spp.
Herd outbreaks of Serratia mastitis have occurred in herds where Serratia grew in bedding and/or teat dip. Poor udder cleanliness and damaged teat ends also appear to increase risk of spreading Serratia to uninfected cows.
How do Serratia spp. infect the mammary gland?
Serratiaspp. infect uninfected cows through environmental contact. As with control of all environmental organisms, maintaining a clean and dry environment for cows is of utmost importance.
Similarly, using inorganic bedding (sand) also reduces environmental contamination by these bacteria.
However, it is important to remember that recycled sand can serve as a source of environmental contamination as organic matter accumulates in the bedding material.
How can mastitis caused by Serratia spp. be prevented and controlled?
Practices for controlling Serratia spp. include implementing proper milking procedures and maintaining a clean and dry housing environment containing appropriate bedding materials.
At milking time, all quarters should be forestripped to begin the milk let-down process. Using an efficacious pre-milking teat disinfectant following forestripping is particularly important in controlling this mastitis-causing pathogen.
Chlorhexidine is not an effective killing agent for Serratia spp.; therefore, producers with herds experiencing Serratia mastitis should choose a pre-milking teat disinfectant containing an alternative active ingredient.
The pre-milking teat disinfectant should remain on the teats for 30 seconds and should be removed with either a paper towel or a single-use clean and dry cloth towel.
When these guidelines are followed, the time from start of manual stimulation (forestripping or wiping) until unit attachment is in the range of 60–120 seconds, an appropriate period of time for milk let-down to occur.
In addition, reducing teat end exposure between milkings, by scraping the back of cow stalls (where the udder rests) and applying fresh bedding frequently, will be worth your time. When herd-wide infection occurs, quick identification of the Serratia source—cows, teat dip, or bedding—is essential to reduce the spread of the infection.
How can teat dip be protected from Serratia contamination?
Although teat dip does not usually contain Serratia marcescens, teat disinfectants can become contaminated with these organisms on-farm. Furthermore, Serratia spp. are commonly resistant to chlorhexidine-gluconate disinfectants.
Therefore, if a container of disinfectant containing one of these active ingredients becomes contaminated, the continued use of this disinfectant on the farm can pose a threat to the rest of the herd. Dairy producers should consider culturing their teat dip if Serratia spp.
is found in more than one cow, and especially if a chlorhexidine-gluconate disinfectant is used as germicide in the teat dip. Moreover, it is important to remember that the product should only be removed from the original container.Leftover teat disinfectant from teat dipping cups should never be poured back into the original container or re-used for a subsequent milking.
When are Serratia mastitis infections most ly to occur?
New infections can occur at any time during lactation and may also occur during the dry period. However, cows in early lactation are at an increased risk for new infections due to the increased stress and immune suppression associated with the postpartum period. Cows with high milk production are not at greater risk than cows with low milk production.
How ly to be cured are Serratia infections?
Serratiais resistant to most antibiotics, and, therefore, cure rates are limited. Thus, intramammary antibiotic treatment is not recommended. Some veterinarians have found limited success with the infusion of sterile saline into the gland.
This treatment acts to alter the osmolarity and, thus, may aid in the elimination of bacteria present in the gland. Veterinary consultation is recommended prior to the start of any treatment protocol.
Due to the limited cure rates with the previously discussed options, emphasis needs to be placed on prevention of these infections, rather than on treatment.
Summary
- Serratiaspp. are environmental organisms found commonly in soil and plant matter.
- It is imperative to keep bedding clean and dry.
- Use of washed sand bedding helps reduce the environmental load of Serratia spp.
- Chlorhexidine-gluconate teat disinfectants are not effective in killing Serratia spp.
- Proper milking procedures are critical in the prevention of these infections.
- Serratiaspp. are resistant to most antibiotics, and, thus, cure rates are limited.
Author Information
Christina S. Petersson-Wolfe, Sandy Costello, and John Currin, Virginia Tech
Источник: https://articles.extension.org/pages/61743/serratia-sppa-practical-summary-for-controlling-mastitis
Serratia marcescens • ru.knowledgr.com
Serratia marcescens — вид грамотрицательных бактерий формы прута в семье Enterobacteriaceae. Человеческий болезнетворный микроорганизм, S.
marcescens вовлечен во внутрибольничные инфекции (HAIs), особенно связанную с катетером бактериемию, инфекции мочевых путей и раневые инфекции, и ответственен за 1,4% случаев HAI в Соединенных Штатах.
Это обычно находится в дыхательных и мочевых путях госпитализированных взрослых и в желудочно-кишечной системе детей.
Из-за его богатого присутствия в окружающей среде и его предпочтения влажных условий, S.
marcescens обычно находится, растя в ванных (особенно на жидком растворе плитки, углах душа, туалетной линии воды и бассейне), где это проявляет как розовое, розово-оранжевое, или оранжевое обесцвечивание и слизистый фильм, откармливающий на убой содержащие фосфор материалы или жирные вещества, такие как остаток шампуня и мыло.
После того, как установленное, полное уничтожение организма часто трудное, но может быть достигнуто применением основанного на отбеливателе дезинфицирующего средства. Полоскание и высыхание поверхностей после использования могут также предотвратить учреждение бактерии, удалив ее источник пищи и делая окружающую среду менее гостеприимной.
S. marcescens может также быть найден в окружающей среде, такой как грязь, предположительно «бесплодные» места и subgingival биофильм зубов. Из-за этого, и потому что S.
marcescens производит красновато-оранжевый tripyrrole пигмент, названный prodigiosin, он может вызвать внешнее окрашивание зубов. Биохимический путь, иллюстрирующий производство prodigiosin S. marcescens, неизвестен за исключением заключительных двух шагов.
В этих шагах (БЕЗУМНЫЙ) monopyrrole и bipyrrole (MBC) подвергается реакции уплотнения посредством фермента сжатия, чтобы в конечном счете сформировать prodigiosin.
Идентификация
S. marcescens — подвижный организм и может вырасти в температурах в пределах от 5–40°C и на уровнях pH фактора в пределах от 5 — 9.
Это дифференцировано от других грамотрицательных бактерий его способностью выполнить гидролиз казеина, который позволяет ему производить внеклеточные металлопротеиназы, которые, как полагают, функционируют во взаимодействиях матрицы клетки-к-внеклеточному. S.
marcescens также показывает деградация соли лимонной кислоты и триптофан. Один из конечных продуктов деградации триптофана — pyruvic кислота, которая тогда включена в различные метаболические процессы S. marcescens. Конечный продукт деградации соли лимонной кислоты — углерод.
Таким образом S. marcescens может полагаться на соль лимонной кислоты как на углеродный источник. В идентификации организма можно также выполнить метил красный тест, который определяет, выполняет ли микроорганизм смешано-кислотное брожение. S. marcescens приводит к отрицательному тесту.
Другое определение S. marcescens — своя способность произвести молочную кислоту окислительным и ферментативным метаболизмом. Поэтому, сказано, что S. marcescens является молочной кислотой O/F +.
Патогенность
В людях S. marcescens может вызвать инфекцию в нескольких местах, включая мочевые пути, дыхательные пути, раны и глаз, где это может вызвать конъюнктивит, кератит, endophthalmitis, и порвать инфекции трубочки.
Это — также редкая причина эндокардита и остеомиелита (особенно у людей, которые используют внутривенные наркотики рекреационно), пневмония и менингит. Большинство S.
marcescens напряжения стойкое к нескольким антибиотикам из-за присутствия R-факторов, которые являются типом плазмиды, которые несут один или несколько генов, которые кодируют сопротивление; всех считают свойственно стойкими к ампициллину, макролидам и цефалоспоринам первого поколения (таким как cephalexin).
В коралле Элкхорна S. marcescens — причина болезни, известной как белая болезнь сифилиса. В тутовых шелкопрядах это иногда происходит как вторичный болезнетворный микроорганизм при вирусной flacherie болезни.
В научно-исследовательских лабораториях, нанимающих дрозофил Дрозофилы, инфекция их с S. marcescens распространена. Это проявляет как розовое обесцвечивание или мемориальная доска в или на личинках, куколках, или обычно крахмал и основанная на сахаре еда (особенно, когда неправильно подготовлено).
Редкая клиническая форма гастроэнтерита, появляющегося в раннем младенчестве, вызванном заражением S. marcescens.
Красный цвет подгузника может быть принят за истинную гематурию (кровь в моче), который может вызвать ненужные расследования врачами.
S. marcescens вызывает curcurbit желтую виноградную болезнь, приводя к иногда серьезным потерям в полях дынь.
Возможная роль в средневековых чудесах
Из-за его красной пигментации, вызванной выражением пигмента prodigiosin и его способностью вырасти на хлебе, S.
, marcescens был вызван как натуралистическое объяснение средневековых счетов «удивительного» появления крови на евхаристии, которая привела к Папе Римскому Урбану IV, устанавливающему Банкет Корпус-Кристи в 1264.
Это сопровождаемое празднование массы в Больсене в 1263, во главе с богемным священником, у которого были сомнения относительно transubstantiation или превращение хлеба и вина в Тело и Кровь Христа во время Массы. Во время Массы евхаристия, казалось, кровоточила и каждый раз, когда священник вытер кровь, больше появится.
В то время как Serratia возможно мог произвести единственное появление красного пигмента, неясно, как это, возможно, произвело больше пигмента после каждого стирания, оставив это предложенное объяснение открытым для сомнения. Это событие празднуется во фреске в Апостольском Дворце в Ватикане, окрашенном Рафаэлем.Присутствие «крови» на хлебе в еврейских домашних хозяйствах, возможно, также использовалось в качестве доказательств, чтобы поддержать так называемую клевету крови.
Открытие
S. marcescens был обнаружен в 1819 венецианским фармацевтом Бартоломео Бицио как причина эпизода кроваво-красного обесцвечивания поленты в городе Падуе.
Бицио назвал организм четыре года спустя в честь Серафино Серрати, физика, который разработал ранний пароход; эпитет marcescens (латынь для «распада») был выбран из-за быстрого ухудшения пигмента (наблюдения Бисио принудили его полагать, что организм распался в подобное растительной слизи вещество на достигающую зрелость). Serratia был позже переименован в Monas prodigiosus и Бациллу prodigiosus, прежде чем настоящее имя Бисио было восстановлено в 1920-х.
Роль в тестировании биологической войны
До 1950-х S. marcescens, как ошибочно полагали, был непатогенным «saprophyte», и его красноватая окраска использовалась в школьных экспериментах, чтобы отследить инфекции.
Во время холодной войны это использовалось в качестве притворщика в тестировании биологической войны американскими войсками, которые изучили его в полевых тестах вместо бактерии туляремии, которая использовалась в военных целях в то время.
26 и 27 сентября 1950, американский военно-морской флот провел секретный эксперимент, названный «Операционные Морские брызги», в которых некоторый S. marcescens был выпущен разрывными воздушными шарами его по городским районам Сан-Франциско область залива в Калифорнии.
Хотя военно-морской флот позже утверждал, что бактерии были безопасны, начав 29 сентября, 11 пациентов в местной больнице заразились очень редкими, серьезными инфекциями мочевых путей, и один из этих людей, Эдварда Дж. Невина, умер. Случаи пневмонии в Сан-Франциско также увеличились, после S. marcescens был выпущен.
(Что бактерии притворщика вызвали эти инфекции, и смерть окончательно никогда не устанавливалась. Сын и внук Невина потеряли судебный процесс, который они принесли против правительства между 1981 и 1983.) Бактерия была также объединена с фенолом и притворщиком сибирской язвы и распылена через южный Дорсет американскими и британскими военными учеными как часть испытаний ИГРЫ В КОСТИ, которые бежали с 1971 до 1975.
С 1950 S. marcescens постоянно увеличивался как причина человеческой инфекции со многими напряжениями, стойкими к многократным антибиотикам. Первые признаки проблем с вакциной против гриппа, произведенной Chiron Corporation в 2004, включили S. marcescens загрязнение.
Загрязненный injectables
В начале 2008, американское Управление по контролю за продуктами и лекарствами выпустило общенациональный отзыв одной партии Предварительно заполненного Решения для Потока Замка Гепарина USP.
Гепарин IV сиринксов потока, как находили, были загрязнены S. marcescens, который привел к терпеливым инфекциям. Центры по контролю и профилактике заболеваний подтвердили рост S.
marcescens от нескольких нераскрытых сиринксов этого продукта.
S. marcescens был также связан с 19 случаями в Алабамских больницах в 2011, включая 10 смертельных случаев. Все вовлеченные пациенты получали полную парентеральную пищу в то время, и это исследуется как возможный источник вспышки.
См. также
Красный подгузник Syndrom. Ребенок преподобного Пэедиэтр. Июль 1960 года; 31:335-9
Источник: http://ru.knowledgr.com/00357271/SerratiaMarcescens

